Resetting the relationship between local and national government. Read our Local Government White Paper
Reducing restrictive practice

Essentials for commissioners of social care services for people with a learning disability and autistic people.
The aim of this document is to provide a briefing for commissioners of social care services for people with a learning disability and autistic people, on the recognition of restrictive practices and the requirements for social care providers to work towards reducing their use of restrictive practices. It also explains the Care Quality Commission (CQC) requirements that when arranging training on the use of, and reduction in, restrictive practices, social care providers must use accredited trainers, and explains what this involves. It is relevant for services for all ages, where they are registered and inspected by CQC.
The aim of this document is to provide a briefing for commissioners of social care services for people with a learning disability and autistic people, on the recognition of restrictive practices and the requirements for social care providers to work towards reducing their use of restrictive practices. It also explains the Care Quality Commission (CQC) requirements that when arranging training on the use of, and reduction in, restrictive practices, social care providers must use accredited trainers, and explains what this involves. It is relevant for services for all ages, where they are registered and inspected by CQC.
Introduction
- Successive investigations into harm experienced by people in health and care services has shown that restrictive practices cause significant risk to people who may not be able to protect themselves from harm, due to their care and support needs. Councils have duties, under the Care Act 2014, for safeguarding people who may not be able to protect themselves from the risk of harm, due to their care and support needs.
- It is therefore essential that commissioners and those monitoring contract compliance of services provided under a council contract are familiar with the requirements on providers who consider the use of restrictive practices, to ensure that training in the prevention and use of restrictive practices is in line with registration and contractual requirements.
Background
In October 2018, as a result of ongoing concerns in the area of restrictive practice, the Secretary of State for Health and Social Care asked the Care Quality Commission (CQC) to carry out a review of restraint, segregation and seclusion of autistic people, people with a learning disability and people with mental health problems. CQC commissioned a review of the use of restrictive practice, resulting in the October 2020 publication “Out of sight – who cares?”, with recommendations for both national bodies and local authorities.
“Out of sight – who cares” included the following recommendation (Recommendation 16), for action by providers:
Providers should review their practice to ensure that restrictive interventions are used for the shortest possible time in line with the National Institute for Health and Care Excellence (NICE) guideline on violence and aggression: short-term management in mental health, health and community settings, rather than using such interventions as longer-term solutions. This should be checked by CQC and NHS England.”
Progress against the recommendations was reviewed in December 2021 and March 2022. The March 2022 review highlighted that recommendation 16 had not been met. It noted that:
“Our Interim report in 2019 and Out of sight report in 2020 highlighted the serious concerns that we had regarding the use of restraint, seclusion and segregation for people with mental ill health, those with a learning disability and autistic people. This was of particular concern in inpatient units, but we found they were also being used in adult social care settings.”
In relation to Recommendation 16, the March 2022 review went on to note from what it had seen and heard:
"There is a continued over-reliance on restrictive interventions. People are too frequently subjected to practices that are about containment and are not therapeutic. Restrictive interventions include restraint, seclusion and long-term segregation.
“It is important to remember that each time a restrictive intervention is used, it has an impact on that person and staff; restrictive interventions can cause further trauma to people and add to feelings of dehumanisation.”
Guidance for commissioners
This briefing is designed to support local authority commissioners of social care support for autistic people and people with a learning disability to understand and recognise restrictive practice in social care, and to understand the CQC requirements of providers so that commissioners can play their part in reducing its use. It is recognised that the NHS may commission services from social care providers. It is also noted that the briefing may be of value to health or education commissioners of services for adults or children. Although the guidance has been specifically developed in relation to services for people with a learning disability and autistic people, it may be relevant to services for other people, that is, who do not have a learning disability and who are not autistic.
Definitions
Various legislative frameworks, statutory guidance and other key documents describe restraint and restrictive practice and provide guidance and recommendations. This includes:
- The Mental Health Act (1983) and its Code of Practice
- The Mental Capacity Act (2005) and associated Code of Practice and the (now archived) Deprivation of Liberty Safeguards Code of Practice
- The Mental Health Units (Use of Force) Act (2018) and associated statutory guidance
- Out of sight: who cares? reports and progress reports from the Care Quality Commission (CQC)
- The August 2023 CQC blog Restrictive Practice: a failure of person-centred care planning?, which incorporated the new CQC policy position statement on restrictive practice
- The Restraint Reduction Network’s Training Standards (v 1.3 July 2021)
- The Restraint Reduction Network’s document Towards Safer Services (v 22), which provides support to organisations to work towards reducing restrictive practice.
- The joint LGA/ADASS joint publication Promoting less restrictive practice - Reducing restrictions tool which supports practitioners working in the context of Deprivations of Liberty authorisations under the Mental Capacity Act 2005, to ensure that the least restrictive options are included in care and support plans, by considering whether there are any less restrictive options possible for an individual, than are being proposed.
- Baroness Hollins’s report (November 2023) My heart breaks - solitary confinement in hospital has no therapeutic benefit for people with a learning disability and autistic people
Many different terms are used for different types of restraint and restrictive practice, often interchangeably. Baroness Hollins’s November 2023 report, which focuses on enforced isolation in hospital, recognises this and, in particular, calls for a single “overarching term to describe the common experience of enforced isolation where people are denied meaningful human contact”. The report uses the term “solitary confinement”, as an umbrella term to mean: “enforced isolation from meaningful human contact with peers which includes all practices that deny people meaningful contact with other people, including but not only, those currently referred to as seclusion, time-out or long-term segregation.”, stating that “this will improve recognition, monitoring, intervention and safeguards for all uses of enforced isolation.” The report recognises that:
“the use of solitary confinement for people with a learning disability and autistic people has the potential to cause significant harm to the physical, emotional and psychological wellbeing of those persons.”
The CQC uses a broad definition in their August 2023 policy position statement (see more information, below), that encompasses restraint and more subtle types of restrictive practice, in an all-inclusive, straightforward umbrella definition of restrictive practice, as follows:
“Restrictive practice is defined as making someone do something they do not want to do or stopping them from doing something they do want to do, by restricting or restraining them, or depriving them of their liberty.”
This brings together various types of restraint and restriction, as well as more subtle types of restrictive practice (see below).
CQC requirements
In August 2023, Rebecca Bauers, CQC Interim Director of People with a Learning Disability and Autistic People, and Chris Dzikiti, CQC Director of Mental Health, published a new CQC cross-sector policy position statement on restrictive practice, in their August 2023 blog. This highlighted that CQC would be prioritising the reduction in restrictive practices and would expect all providers of health and social care to know what restrictive practice looks like, and to actively work to reduce its use in health and care settings.
The CQC policy position statement – August 2023
The CQC policy position statement explains what is meant by restrictive practice and what it looks like, and it expects the use of blanket policies to be challenged.
It recognises that “most people know and accept that restraint, seclusion, and segregation are more extreme forms of restrictive practice. But there are more subtle forms of restrictive practice that easily become day-to-day normal responses to perceived risk or lack of time. There is the risk that without regular review, the use of restrictive practice can increase gradually over time without really being noticed, and passed off as “just the way we do things here”.
The policy statement recognises that “there are limited situations where restrictive practice could be needed to keep people safe. However, restrictive practice must only be used to prevent serious harm. It must be the least restrictive option, applied for the shortest possible time. It must only be carried out with the correct authorisations beforehand. Any incident where restrictive practice is used must be followed by therapeutic support for the person. There must also be a detailed review of their care plan, which focuses on de-escalating and preventing any future incidents.”
Recognising that restrictive practice can itself cause further trauma, the policy position statement states that:
“Wherever restraint, seclusion or segregation is perceived to be the only safe option, providers must consider whether services were provided which met the needs of the individual and are preventative in their approach to stop situations reaching crisis point. This must include considerations of any failures in people’s care, learning or gaps in listening to and understanding people, and the required proactive system wide joined up working. We expect providers to respond to any restrictive practice by organising timely therapeutic interventions for the person/s subjected to the restrictive practice, to address any trauma caused to them, and to support their future wellbeing.”
CQC “expects everyone in health and social care to be actively working towards reducing the use of restrictive practice, to the point where its use is rare, and it is considered a failure of care across a system. In its place, we expect to see regularly reviewed, person-centred, trauma-informed care plans that are tailored to each individual’s specific needs.”
The role of social care commissioners and contract compliance staff
Colleagues in health and social care need to take immediate steps to identify and reduce restrictive practices in services, where possible, recognising the existing requirement for providers to work towards this reduction. This means that staff and other people who visit adult social care services need to be able to recognise restrictive practices and be informed and alert to this issue. Commissioners should be clear with social care providers that they require commissioned services to work towards the reduction of restrictive practices and that they will challenge such practices if, and when, they come across them. Commissioners should incorporate requirements into service specifications, reviewing evidence during tender evaluation and monitoring evidence of practice in contract compliance visits. Commissioners can refer providers to the Restraint Reduction Network’s quality assurance framework Towards Safer Services, to offer support in planning a reduction in their use of restrictive practices.
Commissioning staff may be informed of restrictive practice via the complaints process or from a safeguarding enquiry. They will need to draw together information from a wide range of people, to check whether restrictive practices are being used in social care services in the local authority area. This information may come from a variety of sources:
- people who are supported by a provider (in their own home, or who live in, or visit, a social care setting)
- peer advocates and quality checkers
- family members or friends
- staff employed by the provider
- visiting professionals, health, social care and education practitioners
- CQC or Ofsted inspectors
- statutory or non-statutory independent advocates
- others who meet people during their day-to-day life.
Local authority contract compliance staff may observe practice themselves, and may also routinely share intelligence with other commissioning staff, such as health or education colleagues, and with safeguarding practitioners and inspectors from the Care Quality Commission or Ofsted.
Training for staff on restraint reduction – required certification
In July 2019, a joint letter was sent to the health and social care sector from CQC, NHSE, LGA, ADASS, HEE and Skills for Care to introduce and endorse the Restraint Reduction Network’s training standards and certification scheme on restrictive practices. The letter explained that NHS had commissioned the Restraint Reduction Network to develop standards for training as part of their work to reduce reliance on restrictive practices in mental health units. The standards are designed to apply in services for adults and children, including education and social care settings.
The standards continue to provide a national benchmark for training in restrictive practices and have been endorsed by a number of professional bodies, charities and arm’s length bodies, and the letter stated that “local authority commissioners should now refer to the Restraint Reduction Network Training Standards (instead of the BILD Code of Practice)”, and explained that “training services can be certified as complying with the Restraint Reduction Network Training Standards. Certification must be accredited by the UK Accreditation Service (UKAS) as complying with the ISO standards for certification. UKAS is the national accreditation body for the United Kingdom. UKAS ensures the competence, impartiality & integrity of the certification scheme.”
The letter announced that CQC would expect services across health and social care to use certified training. It was circulated via relevant networks to ensure all relevant professionals, commissioners, service providers, and training organisations were aware of the new standards and certification process. It encouraged commissioners to require, through contracts, that “training services that include restrictive practices are certified (by UKAS accredited body) as complying with the Restraint Reduction Network Training Standards”. It also encouraged “all relevant service providers (across health and social care) who commission training to check that their training provider is working towards certification (that is, UKAS accredited) as complying with the Restraint Reduction Network Training Standards.”.
In November 2020, a further joint letter was sent to all relevant service providers to say that all those who commissioned training in restrictive practice should check that the training is certified, because from April 2021, CQC would expect all services across health and social care to only use training in restrictive practices that is certified as complying with the Restraint Reduction Network training standards.
Certification is via Bild Association of Certified Training. There are three categories of training provider on the certification journey:
- certified training services
- affiliate organisations
- organisations who are working towards certification
Providers and commissioners of health and care services can check whether a trainer is certified on the Bild certified organisations website. They can also check whether a training organisation is currently working towards certification but are not yet delivering certified training. A certified trainer will also have a certificate. If the training is not certified, it is not compliant with CQC expectations.
Social Care commissioners should satisfy themselves during the tendering process that commissioned providers only use training (where training includes restrictive practices) that is certified as meeting the RRN training standards, in line with CQC requirements. Please note, however: this CQC requirement applies in CQC-inspected settings that provide services for children. But where the setting is regulated and/or inspected by Ofsted/DfE only, then CQC would have no involvement and education and social care providers are permitted to use trainers that are not UKAS accredited/certified by BILD, if they wish.
The Restraint Reduction Network training standards
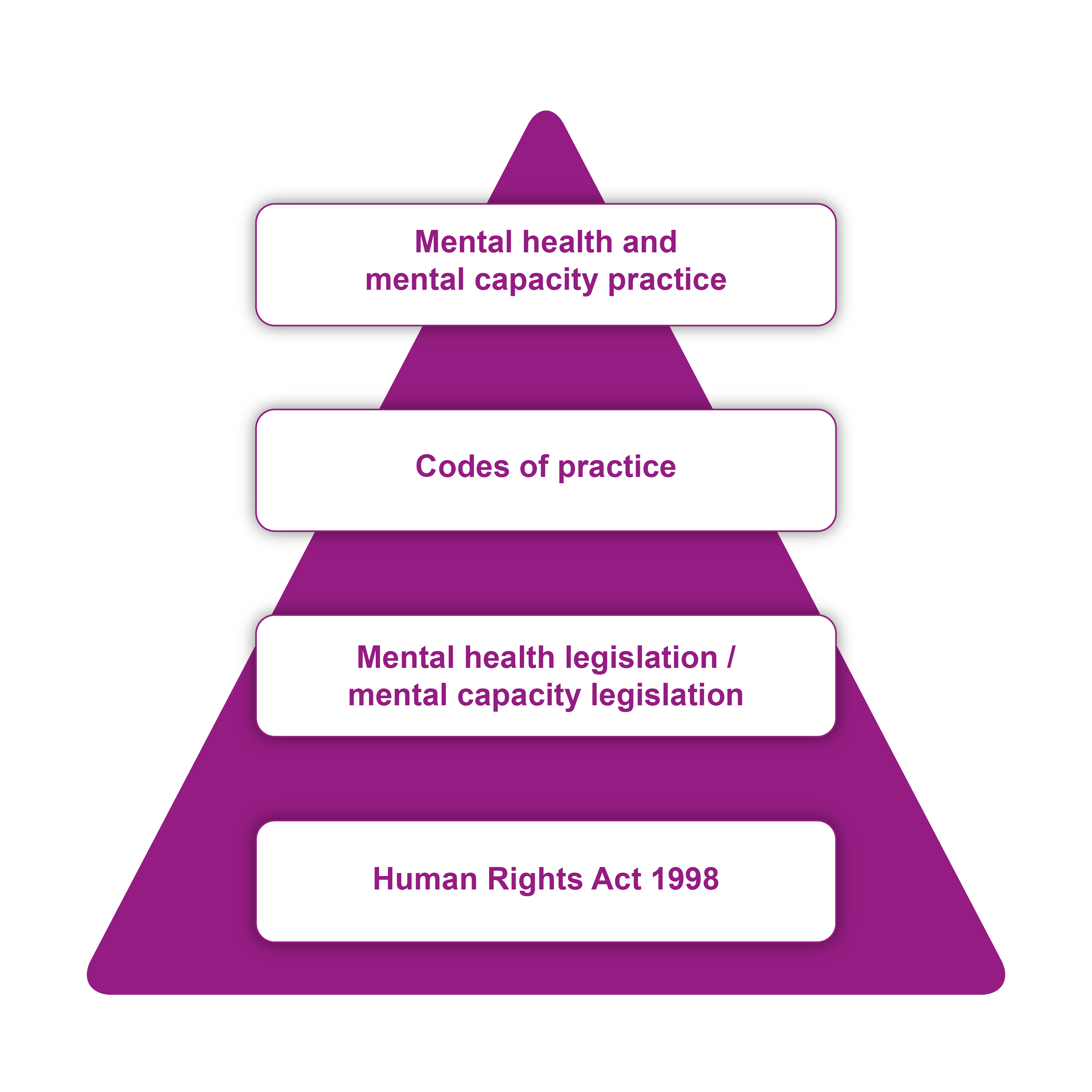
The Restraint Reduction Network training standards emphasise the human rights of people who may be subjected to restrictive practice and explain the relationship between legislative frameworks involved in restrictive interventions. The training standards state that “training must ensure that the relationship between the Human Rights Act and other legal frameworks relevant to the use of restrictive interventions is understood and those laws are applied in a way that is compatible with the person’s rights.” The standards recognises that there are many legislative frameworks involved and that:
Training must make clear reference to how the Human Rights Act 1998 and other key legislation work together in practice. Essentially, other legislation should be interpreted and applied in a way that is compatible with people’s human rights.”
The Restraint Reduction Network (RRN) training standards use a diagrammatic representation based on a diagram in the British Institute of Human Rights (BIHR) 2016 leaflet, 'Mental Health, Mental Capacity, and Human Rights: A practitioner’s guide' to show how the Human Rights Act operates as the foundation for other law, policy, guidance and practice. We've reproduced the diagram:
The independent evaluation of the Restraint Reduction Network training standards by Manchester Metropolitan University, funded by Burdett Nursing, concluded that the training standards provide effective quality assurance of training resulting in improving the quality of training and being an “important contributor towards a wider organisational cultural shift needed”.
Good practice
The Mental Health Units (Use of Force) Act (2018) and associated statutory guidance places requirements on mental health hospital units, but much of what it requires from mental health units would be considered as good practice for other health, social care and education services. It would also be good practice to broaden the requirements to include less obvious, subtle restrictions, as well as the more obvious restraints and use of force. Social care commissioners should consider whether to include the following in contracts:
- A responsible person should be appointed whose duty is to oversee the use of restrictions (including use of force) in all services of an organisation
- Providers should have a restraint and restrictions policy – and this should be developed in consultation with people who draw on the services or support and other relevant people
- Providers should publish information, and provide a copy to all people who draw on the support or service, on their rights in relation to restrictions and the use of force – developed in consultation with relevant people
- Training that includes restrictive practices should be certified as meeting the RRN training standards
- Data should be recorded on any restrictions
- Data should be kept for three years and monitored by senior managers or the Board annually.
- There should be an annual report about deaths that have been reported to the coroner
- Deaths should be referred into the LeDeR process
- Serious injuries should be investigated
Note that if the police are called to an incident, they may wear and switch on a body-worn video device (also referred to as body-cams) to independently capture what is seen and heard (note that under the Mental Health Units (Use of Force) Act (2018), if a police officer goes into a mental health unit on duty to assist staff who work in that unit, the police officer must wear and operate a body camera at all times when reasonably practicable).
Resources
Partners in care and health (PCH) resources
You can find published resources from our people with a learning disability and autistic people team, via our webpage on Autistic people and people with a learning disability.
Closed cultures in social care: a guide and questions to ask
Other useful resources
Right support right care right culture (pdf). This is CQC’s statutory guidance on 'How CQC regulates providers supporting autistic people and people with a learning disability,' and includes key principles.