In late 2017 the Technology Enabled Care (TEC) team began working on a project to improve pathways and access to TEC for those who were being discharged from hospital. The aim was to significantly increase the take-up of lifelines and telecare within a vulnerable cohort that would most benefit from them and ensure that people had access to the councils in house Reablement Enhanced Response Service (ERS). This example of a local initiative forms part of our managing transfers of care resource.
Cambridgeshire County Council’s Technology Enabled Care (TEC) is provided by a central team that is jointly funded by the local authority and Cambridgeshire and Peterborough clinical commissioning group.
In late 2017 the team began working on a project to improve pathways and access to TEC for those who were being discharged from hospital. The aim was to significantly increase the take-up of lifelines and telecare within a vulnerable cohort that would most benefit from them and ensure that people had access to the councils in house Reablement Enhanced Response Service (ERS).
The purpose of the project was twofold. Firstly that anecdotal evidence from colleagues suggested that timely access to this equipment causing delays, with no lifelines or key safes being in place at the point of discharge. In addition patients’ families were expected to make these arrangements themselves at a time of potentially great stress. This was exacerbated by a complex telecare market with multiple providers throughout the county.
Secondly in cases where there was no telecare the risk of readmission within 48 hours was greatly increased. For example an overnight fall may not be identified in time and would potentially result in an admission that could have been prevented if it was acted on sooner.
The plan
To help service users overcome the complications of referral and installation for service users and their carers Cambridgeshire TEC has offered a custom telecare discharge package. This includes installation and rental of the lifeline for six weeks, alongside any other pieces of appropriate equipment such as smoke alarms, temperature sensors and fall detectors.
The project itself was funded through part of a successful bid to the local authority’s Transformation fund to support the increased use of TEC to support the whole system.
At the end of the six week trial period the person has a choice of continuing to pay for the package’s line rental themselves, usually three to four pounds a week or to have the system removed.
For certain cases a ‘Just Checking’ activity monitoring service is also installed in the service user’s home. For a period of time sensors would track their activity around the premises. This establishes a better understanding of their needs and provides evidence towards determining the most appropriate intervention for that service user.
All participants also have access to the county’s ERS team which responds to telecare alerts and people who require non-emergency assistance; providing an alternative to an ambulance call-out when possible.
Implementation
Referral pathways already existed between TEC and the Discharge Planning Teams. Although referral rates were often low. Therefore the implementation of the trial was mostly a case of promoting the new kind of service provision amongst the various teams.
From the outset of the trial, as well as internal resource Cambridgeshire TEC worked with a local telecare monitoring centre to ensure that there was sufficient capacity for the number of expected installation and potential uninstallations at the end of the six week trial. This required amendments to the service level agreement between the two organisations to establish clear parameters for the new kind of service provision.
Over 2018 the telecare monitoring centre was responsible for 199 (70.3 per cent) of installations with an average cost of £99.78 per installation. Meanwhile Cambridgeshire TEC team was responsible for the remaining 29.7 per cent with an average cost of £35.49 per installation. Both of these sets of costs were covered by Cambridgeshire TEC.
Whilst the trial was initially exclusive to hospital discharges access was soon extended to other teams such as Reablement (April 2018) and Adult Early Help (October 2018), many of whose service users were identified as having the qualities which would benefit from Technology Enabled Care. Again, this extension was coupled with a similar promotion campaign as when introducing the scheme to hospital discharge.
Outcomes
Referrals and retention
Over 2018 282 service users took part in the trial, making up 9.9 per cent of all referrals for that year. The number of installations per month ranged from as low as 7 in March to a high of 44 in December, with a general trend upwards as more teams were allowed to access the scheme.
Of the 273 service users who have completed their trials between 1 January 2018 and 31 January 2019 190 continued with their telecare provision following the installation of their lifeline, a retention rate of 69.6 per cent.
A particular area of success was when Reablement were introduced to the pilot in April. The number of referrals for the trial reached a peak of 40 per cent of all Reablement referrals in August 2018. This was coupled by a significant increase in the number of Reablement referrals to Technology Enabled Care in overall, from a low of 3 per cent of all referrals over February and March to a high of 19 per cent of all referrals in August. For Reablement, the trial had contributed to an environment where it is seen as easier to refer to Technology Enabled Care overall, not just for the six-week trial.
ERS callouts
Over 2018 54 service users took advantage of ERS with 174 callouts throughout the year. The average number of calls per month for a service user varied from a high of 5.5 to a low of 0.09 calls.
Of these calls 121 (69.5 per cent) were judged to have avoided a further call out from an ambulance. 72 of these resulted in some form of care being provided, from assistance from the floor following a fall (45 calls) to instances of personal care (6).
The majority of responses to the calls were prompt, with 67.2 per cent meeting the target of under an hour. For the 55 calls where assistance from the floor or mobility assistance was required the target was met 89.1 per cent of the time.
If these individuals did not have access to ERS through the trial there was a high possibility that either an ambulance would have attended unnecessarily or a person will have been left on the floor for an extended period of time. In the latter case this would have further increased the risk of the complications such as pressure sores, carpet burns, dehydration, hypothermia, pneumonia and even death.
JCAT results
Out of the 282 service users 20 had a JCAT assessment that started during or after their six week trial.
Whilst not explicitly linked to the six week trial the results provide an insight into how individual service users were behaving. It should be noted that before the deployment of the JCAT that 19 out of 20 were considering a formal escalation in care.
Following the deployment, only two resulted in an escalation in the care package, one of these being a transfer to 24 hour care. There were two cases which resulted in a formal reduction of their care packages. The remaining JCAT studies indicated that there had been no formal increase in the care package.
Instead 13 out of the 20 deployments recommended an increase or maintenance in the provision of telecare, something that was being provided by the trial itself.
Potential preventative savings
The TEC team currently calculates preventative savings through an outcomes based model. The table below lays out some of the outcomes that TEC can help achieve, and the associated costs avoided.
- Desired outcome: Hospital prevention – intervention will raise an alert that the person is experiencing difficulties which if unattended could result in harm to the person
- Social care avoided: Hospital discharge – Average cost of one hour of reablement,£34; average length of package x 21 hrs
- Cost: £714 one off
- Desired outcome: Residential care prevention - intervention will potentially delay or eliminate need for this type of care.
- Social care avoided: average cost of high level care package – might be care home or 24 hour live-in care
- Cost: £750 x18 p/wk (average length of time for which an escalation in care has been delayed because of a TEC intervention is 18 weeks.)
- Desired outcome: Reduce or eliminate care package – intervention will reduce, delay or eliminate formal care required eg waking night care
- Social care avoided: Difference between average cost medium level care package: three to four calls a day £232.26 and average cost of a high level care package might be care home or 24-hour live-in care £750
- Cost: £517.74 x18 p/wk (average length of time for which an escalation in care has been delayed because of a TEC intervention is 18 weeks.)
- Desired outcome: Falls prevention plan – intervention will prevent a fall/hospital admission associated with a fall specifically
- Social care avoided: Hospital Discharge – Average cost of one hour of Reablement £34 Average length of package x 21 hrs
- Cost: £714 on off
Considering the average costs of an installation, the potential savings generated from the prevention of one fall or hospital admission for an individual more than makes up the cost of multiple trials.
Difference in increase in care package over time
Two hundred and fifty-one of the 283 trial participants have some kind of presence on Cambridgeshire County Council’s wider adult social care system. The table below details the split between those on the trial who had an increase, no change or decrease in their care package following the trial, as well as the average weekly increase in care for those individuals.
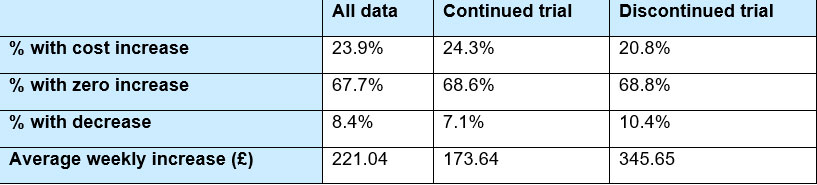
For context, 67 per cent of these participants continued with the trial whilst 33 per cent did not. The cost in care increases apply for all care, even that beyond the 18 week delay mentioned in the section above.
Whilst a higher percentage of those who continued with the trial were subject to some kind of increase in the cost of their care it is also the case that the average increase was half of that than those who discontinued with the trial. It is difficult to attribute this solely to the TEC intervention but the information is nonetheless compelling.
Next steps
The six week lifeline trials have been a great success both increasing referrals to TEC and managing demand for care. The trials have also integrated into other TEC projects such as a trial on ‘Next Generation’ intelligent lifelines. This new system is designed to detect and alert to changes in a service user’s behaviour and daily routine by using motion sensors and machine learning to prevent escalation to a health or social care crisis. This project has recently started and is funded by NHS England.
Case studies
Feedback from service user’s husband who has been provided a lifeline
The gentleman expressed how the lifeline had made a huge difference to his general wellbeing and his role as a carer. He explained that he was previously not able to leave his wife for fear of her falling, saying that now ‘at least I can go out for an hour’.
Woman with Next Generation technology installed
One night an alert was sent by a trial system at 03:08 for a woman living on her own, notifying that the main door had been left open. The primary contact was called as were ERS, both were unable to attend so the police were called. The police arrived to find the property was vacant and they instigated a high risk missing person alert.
The police called back at 04:59 to inform they had located the woman and returned her to the property. The ERS had arrived on site at this point and they worked with the police to settle the lady.
Man with fire in the house
A gentlemen was provided with a lifeline and smoke detector as a part of the six week trial. Soon after there was a house fire, which triggered the smoke detector and lifeline. Fire fighters were able to promptly attend to the blaze and prevent it from spreading to other residences.
If the telecare system was not installed there is a significant chance that emergency services would not have attended in time and he would have not survived.